10th Century B.C., The Oldest Record of Epilepsy
The "Sakikku," a medical document written in Babylonian cuneiform, has the earliest complete description of epilepsy.

International Epilepsy Day is a yearly event co-organized by the International Bureau for Epilepsy (IBE) and the International League Against Epilepsy (ILAE) to raise awareness about epilepsy and its impact on individuals, families, and communities worldwide. It falls on second Monday of February and for year 2023, the day will be celebrated on 13th February.
These are a group of disorders of the CNS characterized by paroxysmal cerebral dysrhythmia, manifesting as brief episodes (seizures) of loss or disturbance of consciousness, with or without characteristic body movements (convulsions), sensory or psychiatric phenomena. These episodes are unpredictable and their frequency is highly variable. Epilepsy has a focal origin in the brain, manifestations depend on the site of the focus, regions into which the discharges spread and postictal depression of these regions. Recognised from the dawn of history as ‘disease of lightening’, it was correctly described by JH Jackson little over a century ago.

One of the oldest known medical diseases in the world, epilepsy has been documented from the dawn of written history. it was viewed as a spiritual issue back then. A person who underwent an exorcism while being possessed by a moon deity is mentioned in a prehistoric Mesopotamian manuscript from 2000 B.C. Seizures were ascribed to demonic possession by the ancient Babylonians. Epilepsy was seen by the ancient Greeks as a form of spiritual possession, but they also connected it to genius and heavenly interventions.
Epilepsy stigma is a historical issue as well. People in ancient Rome did not share plates or pots with those who had epilepsy whether they were eating or drinking. In several regions of Africa up until the second half of the 20th century, epilepsy was thought to be contagious and the result of possession, witchcraft, or poisoning.
Today, more than 120 nations throughout the world observe International Epilepsy Day.
Epilepsy is broadly classified into generalized and partial epilepsies.
 Generalised seizures-
Generalised seizures- 
Tonic spasm of all body muscles—clonic jerking followed by prolonged sleep and depression of all CNS functions.

Momentary loss of consciousness, patient apparently freezes and stares in one direction, no muscular component or little bilateral jerking.

Unconsciousness with relaxation of all muscles due to excessive inhibitory discharges. Patient may fall.
Partial seizures- 

Convulsions are confined to a group of muscles or localized sensory disturbance without loss of consciousness.

Attacks of bizarre and confused behaviour and purposeless movements, emotional changes lasting 1–2 min, and impairment of consciousness.

The partial seizure occurs first and evolves into generalized tonic-clonic seizures with loss of consciousness.
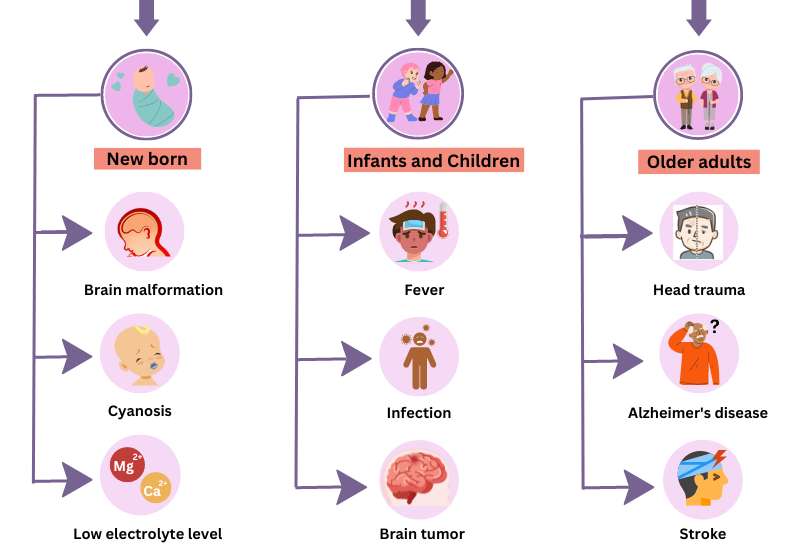
Epilepsy is not contagious. Although many underlying disease mechanisms can lead to epilepsy, the cause of the disease is still unknown in about 50% of cases globally. The causes of epilepsy are divided into the following categories: structural, genetic, infectious, metabolic, immune and unknown. Examples include:

Brain Damage

Stroke

Severe Head Injury

Brain Infection

Congenital Brain Malformations

Brain Tumour
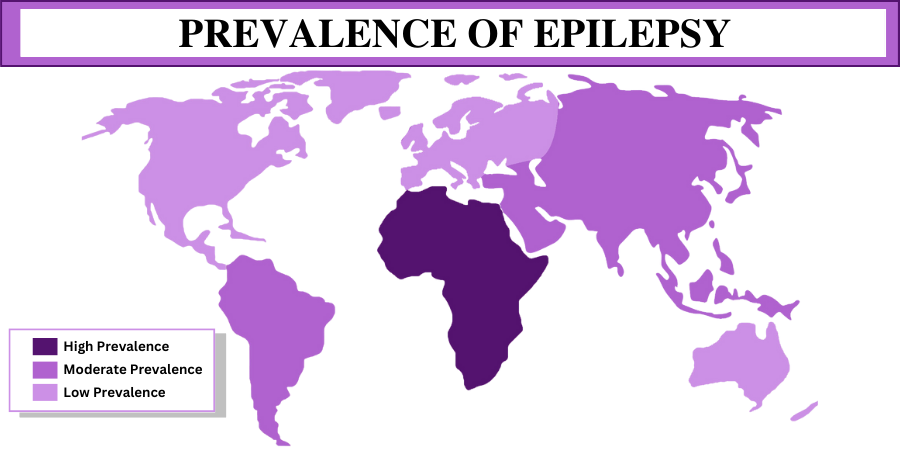
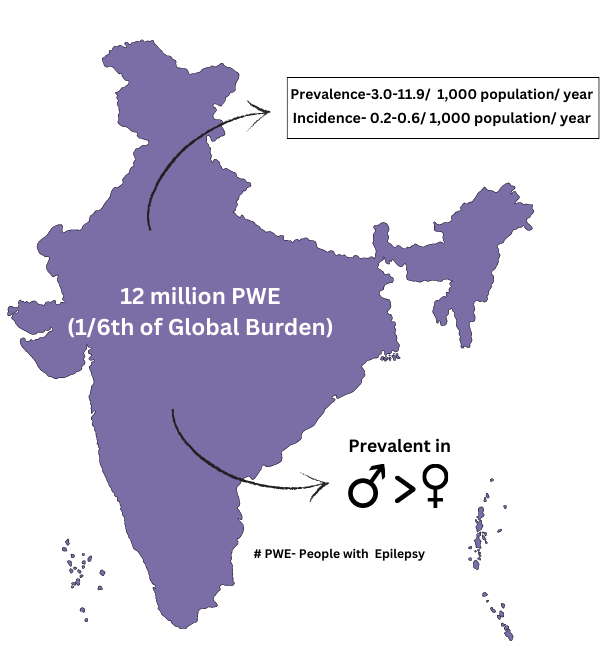
Of the 70 million persons with epilepsy (PWE) worldwide, nearly 12 million PWE are expected to reside in India; which contributes to nearly one-sixth of the global burden
nearly 12 million persons with epilepsy (PWE) are expected to reside in India; which contributes to nearly one-sixth of the global burden.
The overall prevalence (3.0-11.9 per 1,000 population) and incidence (0.2-0.6 per 1,000 population per year).
More men than women have epilepsy. Children and adolescents are more likely to have epilepsy of unknown or genetic origin. Brain injury or infection can cause epilepsy at any age. The Epilepsy Foundation also reports that 70 percent of children and adults with newly diagnosed epilepsy can be expected to enter remission after having gone five years or more without a seizure while on medication.
A doctor makes his or her epilepsy diagnosis based on symptoms, physical signs and the results of such tests as an electroencephalogram (EEG), computed tomography (CT or CAT scan) or magnetic resonance imaging (MRI). The routine protocol followed to diagnose a patient with epilepsy are

The medical history is the foundation of the diagnosis of epilepsy. The doctor needs ALL the information about what happened before, during, and after your seizures. If you cannot give enough information, then others who have seen the seizures happen should contribute what they know. If some of the details are vague, the doctor needs to know that too.

Routine blood studies are indicated to identify the more common metabolic causes of seizures such as abnormalities in electrolytes, glucose, calcium, or magnesium, and hepatic or renal disease. A screen for toxins in blood and urine should also be obtained from all patients in appropriate risk groups.

The electrical activity of the brain (the EEG) is easily recorded from electrodes placed on the scalp. The characteristics of the normal EEG depend on the patient’s age and level of arousal. The rhythmic activity normally recorded represents the postsynaptic potentials of vertically oriented pyramidal cells of the cerebral cortex and is characterized by its frequency.

Almost all patients with new-onset seizures should have a brain imaging study to determine whether there is an underlying structural abnormality that is responsible. MRI has been shown to be superior to computed tomography (CT) for the detection of cerebral lesions associated with epilepsy. In some cases, MRI will identify lesions such as tumors, vascular malformations, or other pathologies that need urgent therapy.
An estimated 25% of epilepsy cases are preventable.
Preventing head injury is the most effective way to prevent post-traumatic epilepsy.
Adequate perinatal care can reduce new cases of epilepsy caused by birth injury.
The use of drugs and other methods to lower the body temperature can reduce the chance of febrile seizures.
The prevention of epilepsy associated with stroke is focused on cardiovascular risk factor reduction
In low and middle income countries elimination of parasites and education on how to avoid infections can be effective ways to reduce epilepsy worldwide
Therapy for a patient with a seizure disorder is almost always multimodal and includes treatment of underlying conditions that cause or contribute to the seizures, avoidance of precipitating factors, suppression of recurrent seizures by prophylactic therapy with antiseizure medications or surgery, and addressing a variety of psychological and social issues. Treatment plans must be individualized, given the many different types and causes of seizures as well as the differences in efficacy and toxicity of antiseizure medications for each patient. In almost all cases, a neurologist with experience in the treatment of epilepsy should design and oversee implementation of the treatment strategy. Furthermore, patients with refractory epilepsy or those who require polypharmacy with antiseizure drugs should remain under the regular care of a neurologist.

