Fetal Sex Disclosure : Do we need alternative view on PCPNDT Act?
Introduction
The global identity of the ultrasound as a miraculous modern pan-medical, cost-effective diagnostic modality has been cloaked in India since its ability to select gender of fetus became synonymous of female feticide. The country has changed in its economics, use of luxurious goods, education, number of medical institutions and administration but evolution could never be reflected on those who proposed the PCPNDT Act and the control of Ultrasound as one and only tool to change the fate of female fetus.1
We will see in discussion that how we are downgrading the critical care medicine by leaving aside concept of 'Golden Hour intervention' due to biased views and unscientific approach.
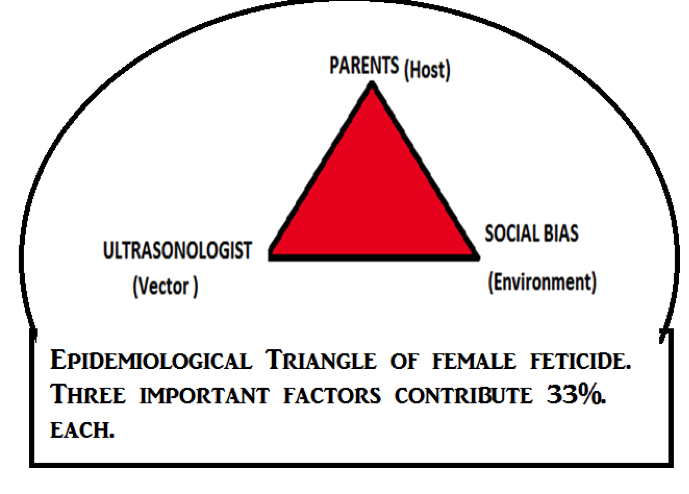
The Model of the Epidemiological Triangle of female feticide
Agent (Ultrasound and doctors) vs. Parents (Host) vs. society (Environment): In my previous article I proposed the model of epidemiological triangle to be applied to female feticide as it has a status of social illness, to understand the 'cause and effect' relationship.2
[caption id="attachment_14780" data-align="aligncenter" data-width="420"]
{kind=link}
Interestingly, the doctors who once were equated to God as the saviour of mankind from diseases, became perpetrator of crime and entered in the triangle as the AGENT, parents as the HOST and family and society as the ENVIRONMENT (Figure1). )It was argued in the theory that despite the complete withdrawal of doctors or ultrasound machines who contributed 33% of the evil practices in triangle, vulnerable major share-holders will continue to contribute to the numbers of missing daughters by sliding the date of execution of homicidal practices after the birth i.e. the female infanticide.2 This argument cannot be waived off as unfounded since there are enough evidences to show that female infanticide existed morbidly before, and incidence gone down with the onset of female feticide. But before envisaging this extreme, one must know that PCPNDT Act is not yet arrived to the stage where physical direct evidences can be collected and culprit doctors can be prosecuted unless activists, administrators or journalists go for sting operations. None of fruitful nabbing of offenders can be attributed to the routine use of Act. 4,5 In the era of flexible morality, administrators and parents who are reflecting social psyche, are being treated as the sanctimonious to the extent that they are not burdened with any accountability for illegalities. That's why, time and again, medical fraternity has been raising voice that PCPNDT Act is actually vilifying them in society.
Ultrasound : (Point of Care Ultrasound) Saving the golden hour in any Emergency:
The Point-of-Care (POC) ultrasound is the limited use of ultrasound technology by non-sonographers to answer specific questions related to patient care needs.
Before peeling the PCPNDT into its virtues and biases, let's examine the emergency use of mobile Ultrasound units during the accidents, natural disaster, cardiac arrest etc (Table1) .
Concept of emergency 'golden hour' in medicine is the key to save all critically sick patients in aforementioned categories. 6,7 After the genocidal war in Rwanda, a small country of Africa lurched because of critical shortage of physicians. How they excelled within their limited resources, is also a success tale of justified and vigorous use of mobile units with ultrasound machines and trained physicians. As a national health policy, the physicians are trained in all remote areas under the TOT (training of trainer) program run by PURE (Physicians for ultrasound in Rawanda Education).8 My own experience about children with cardiac ailment is quoted in the segment of "History.2 Omnipresent USG is now recommended in every emergency management protocols like- trauma medicine, cardiac and non-cardiac intensive care units. It is well documented that ultrasound reduces 'triage to intervention time' drastically. 6,7
By virtue of, restrictive PCPNDT Act, India is in a retrograde route to ancient medicine. An accident at ring road will bring an Ambulance and a doctor with stethoscope but not the ultrasound machine and the expert. In absence of critical evidence based diagnosis, early hepatic, splenic or any other internal bleed would be missed. A vagabond shifting would be only option until an ultrasound expert as well as ultrasound machine registered against him/her would be found in a PNDT certified place in a given range of distance. Who will take blame for sub-optimal outcome and loss of life in that case?
PCPNDT Act has blocked the road for any efficient mobile unit without owning any
responsibility for the regression of critical care facilities in India to an abysmal low.
Arguably, is there any debate exist in the courts, where a serious view point of a committee of specialists had been asked about the counter-productive effects of the ban on ultrasound?
This is the reason why PCPNDT ACT despite of its pious objective, stands on single goal: Crack down on service providers! Where is the acknowledgement in court petitions and orders that ultrasound has grown into omnipresent single modality which matches with stethoscope, ECG, X-Rays, CT Scans, Cath procedures, MRI, biopsy in sensitivity and specificity for any given patient with critical state and yet remains radiation free, mobile and cheap?
History
Sex determination and population control: As reported in the one of the recent publication, in seventies, the preferential fetal sex selection done by amniocentesis, was technically offered to the parents as a cheap and handy option to downsize their family, presumably, steered by western apprehension of 3rd world's population explosion.2,9,10,11 Apparently, the vicious practice started probably with visit of Mr Sheldon Jerome Segel in 1960s, who helped in establishing the family-planning clinics for integrated infertility therapy as well as pre and post-natal care, in All India Institute of Medical sciences, New Delhi, India. 2,9,10,11 Historically, the role of ultrasound in deciphering fetal anatomy was identified in 1968.12,13 Predictably, ultrasound as a non-invasive tool took over the amniocentesis, within the premises of premiere national institute, probably with government approval and international funding. In 1969, sex determination was included as one of the 12 new strategies for global birth control in an international workshop. 9,10,11
MTP Act Ally in female feticide?: Abortion was legalised by the Medical Termination of Pregnancy (MTP) Act (1971) and subsequently became the instrument for fertility control and sex selection. MTP act 1971 included the failure of contraception eligible for MTP under section 3(2) explanation 2.14 Till then no one was talking about the child rights, obviously debate about "Fetal Right" could not be contemplated. With the commercialization of medical profession, handy ultrasound became a money laundering tool leading to the mushrooming of private clinics in Punjab and Haryana, openly calling for sex determination of fetus as a future investment of money- "Spend 1000/ today and save 100000/ later."
In 1994 under the instruction of honourable High Court parliament implemented pre conception-prenatal sex determination test (PCPNDT) Act.1
Spandan- A Program with the help of portable Echocardiography machine for underprivileged, unaware children with heart defects: In 2003, I conceptualised a program "SPANDAN" under NGO-Sanatan dharm Yagya Seva Samiti, with the help of Red Cross Society, Rewa (Local Administration), Madya Pradesh, for guidance and treatment of children.2 The Program became an inspiration for an elaborate ambitious scheme for children with heart diseases by the state government, known as "Atal Bal Hriday Upchar Yojna" under which every child below 14 years of age was assisted by state government of Madya Pradesh to continue these free camps at doorstep. I bought a portable echo machine for free services to the society and eventually landed into the web of PCPNDT Act. I have seen closely and since I had tried to question the inbuilt indiscretion of the system.
PCPNDT Act and Point of care Ultrasound
The above mentioned Act passed in 1994 came into force with effect from 1st January1996 Act amended in 2003. Act was called as "Prenatal diagnostic techniques (Regulation and Prevention of Mis-use) act 1994". Now it is called as "Pre-conception and Pre-natal diagnostic techniques (Prohibition of sex selection) Act, 2003". 1
Undoubtedly, this Act is an important mile stone. It started with being prohibitive to a logical extent. For the first time government made a consistent effort to register thedoctors and machines. The narration of Act is descriptive and includes eight chapters andeight forms. This act also gives guidelines for formation of a supervisory board. The PCPNDT Act takes serious view on mobility of ultrasound machines. 15,16 We will examine the possible reasons behind the unimpressive results of this act.
The Indian Union Government on 9 April 2011 reconstituted the Central Supervisory Board extending its strength of members to 35. Now there will be invited representatives of IRA (Indian Radiological association) and IMA (Indian Medical association)17
PCPNDT Act - Virtues
The Act was further strengthen following a public interest petition filed by the centre for the Enquiry of Health and Allied Themes (CEHAT), the Mahila Sarvangeen Utkarsh Mandal (MASUM) and Dr.Sabu George, who had done extensive research in this area. Female feticide was a great concern. This Act started a new moment which led to aggressive persuasion by government and courts. This brought out public awareness and novel schemes targeting to salvage the female fetus and to benefit the girl child.
PCPNDT Act Biases
a. PCPNDT Act does not acknowledge Parent's susceptibility and social conduciveness as the main culpable crime and doctors are addressed as 'committed offenders' unless they prove themselves, innocent. One must not forget the Dowry system one of the important factor for social disinclination to the birth of a daughter, can be justifiably attributed to the internalised submission of law protectors - like IAS, IPS officers, judges, doctors, lawyers, to the system.18-20 PCPNDT Act depends on these biased minds for execution and implementation of law. There are alternative methods of sex selection and will become prevalent once USG takes back seat.21-23 Interestingly, a reverse medical tourism is happening towards the ASEAN countries for preconception selection of sex silently due to unaddressed anomalous thought process.
Arbitrary selection of members of Central supervisory board: The government has restructured the central supervisory board. Unfortunately the elected members are not the representative of the service provider segment of doctors. For example, paediatricians hardly perform sonography but cardiologists perform echo in almost every case. There is no clear definition of 'eminent' anywhere in Act, so selection of members is arbitrary and not on the merit grounds.7
c. The Act Ignores the late evolution of 'Point of Care Ultrasound': Furthermore, this Act fails to concede that ultrasound has taken entirely different platform and failed to grow vis a vis technical advancement (see table-1).
d. The form A needs to be more accommodative: Form A do not provide separate recognition to the critical care doctors like cardiologists or anaesthetists, trauma specialists who are not trained in fetal ultrasound and do not perform the test.
e. Affidavit needs to be more truthful: "I will not do prenatal sex determination because it is a culpable crime." This statement brings this population of physicians who are untrained in sex determination under the same umbrella of trained sonologists and indirectly attaches them with the skill of test. The fact is, they cannot do it because they are not trained for it.
This is obvious that there is prevailing ignorance in the provision of Act for the thin line drawn between the technical abilities of the group of users.7
f. The lack of statistical comparison between the use vs. misuse, bane vs. boon of ultrasound: There are no published scientific paper to associate PCPNDT Act and improving Sex Ratio. Neither has it been subjected to the evaluation of harm done to critical care practice in India.
g. Act harbours an inherent bias that sex determination is synonymous with female feticide and doctors are inherently criminal-minded: Sex determination, by amniocentesis or by ultrasound, almost gained a policy status and was not illegal for more than 20 years. Criminality of test was truly established only after 2003. Until then the procedure was innocuous professional tool and brought a respectful earning for private Ultrasound clinics. Obviously, these law-abiding doctors were never given a chance to depart gracefully, on call of their own conscience rather they were enforced with law which equated them to the Dowry accused. For example pre-implantation sex selection for family balancing was scientifically published in 2002 by Malpani et al. In a prestigious journal.24
h. Inadvertent advertising by government to improve acceptability of ultrasound as accurate tool for sex determination: The strategists entrusted to implement Act also are the part of advertising the ultrasound mediated sex determination as the error free, inadvertently. Fact is that a first trimester scan has 45% chance and 18 weeks scan 3-4 % chance of assigning female sex to a male baby.25
i. Absence of involvement of the democratically elected professional bodies in decision making and implementation: The professional bodies- IRA and IMA are now special invitee in the board but unfortunately they do not represent the contemporary medical fraternity providing POCUS.
All of above facts reiterate that PCPNDT Law is taken as Gospel-Truth which neither can be questioned nor can be challenged or brought into the scientific scrutiny. Furthermore, any amendment will bring further tightening of noose on the neck of doctors because parents, families are not considered intelligent enough so that they can be accountable for crime equally if not more than the doctors.
Disclosure Of Fetal Sex: An Evolved Medical Practice To Be Sacrificed OnTraditional Bias Of Proponents of PCPNDT -
Globally, studies have been done to prove medical importance of sex determination:
To predict the occurrence sex linked disorders in predisposed families.
- To make family comfortable so that they can plan the house, dresses ambience of place according to the sex of a baby.
There is success rate of 93 – 99 sensitivity for the recognition of male sex in a scan after 17th week. While reported error of assigning female sex to male sex at 12 weeks gestational age is up to 45%.25 So when Union Minister Mrs Maneka Gandhi made a statement regarding the disclosure of the sex of baby, a huge roar of hue and cry greeted her, so much so, that she had to issue a clarification on the matter.
Issue of Burden of Congenital anomalies in a Society without a Security System:
According to the WHO, an estimated 276000 babies die within the 4 weeks of birth, due to congenital anomaly. The 18th week anomaly scan provides the information about life threatening congenital anomalies with sensitivity in the range of 54-99%. India bans easily available diagnostic modality, does not have adequate and affordable transportation facility from remote areas, and few and far tertiary care centres mostly in private hospitals. We need prenatal detection of those diseases where severe disability is expected despite of adequate management. It helps in preparation of family in terms of finances and man power. Also MTP can be opted in seriously debilitating diseases. Ultrasound is main tool for prenatal fetal anomaly scan.
Alternative view on PCPNDT Act:
In a write-up sent to IRA Secretary Dr Jignesh Thaakkar in March 2012, few measures were suggested by me which were forwarded to the medico-legal cell. Subsequently, a letter was written by Dr MC Gupta incharge of medicolegal cell to the Maharastra Medical Council, which had somehow, endorsed my views. Obviously, PCPNDT Act had not achieved its goals in more than 10 years and needed to be scientifically reviewed and some alternative suggestions were needed to be entertained. I had opportunity to publish them and also discuss them in all big or small platforms.2,26 We conducted a debate on PCPNDT Act in the international workshop organized at Fortis Escorts hospital New Delhi 31March - 2nd April 2013. It was attended by eminent users of the point of care USG. Most important guest of this forum was Mr Sabu George, who obliged us by accepting our invitation but did not conceded to any of our arguments. Following were the suggestions which needed a serious consideration:
1.The informers must be encouraged by providing cash reward .
- Registration of pregnancy within 3 months to for eligibility for various othergovernment policies like "Ladli Beti Yojna"
Fetal Sex declaration in Form 'F' .PCPNDT act is all about maintaining the record and informing the PNDT authorities from a registered place. Doctors have been declared the offenders unless proved otherwise, which means, they would not respect their declarations on affidavit. Obviously PCPNDT Act remains a paperwork done cleverly. It is unrealistic to say sex was not detected in 'fetal anomaly scan' because an anomaly scan needs certain views which are bound to reveal sex, unless the "Safe Ultrasound" technology which does not allow imaging of genitals is incorporated in the ultrasound machines.27 This technology exists and patented by all major share-holders of market in USA.27 Within present constrains, mandatory 18 weeks scan and an official information to PNDT office help in following way: a. It will make PCPNDT Act more accountable and scientific because it will bring in PNDT office, ASHA workers and families in the loop; b. It will avoid conveying message to family by simple methods like gesturing, whispering or by the selection of sex of escort taking lady out of clinic; c. 18 week anomaly scan will allow to screen the birth defect like Down's Syndrome.
Mushrooming of institutions claiming rapid certificate courses must be prohibited.
The professional bodies must be made accountable for wrong-doing of their members.
Avoidance of seesaw practice of giving recognition to a training centre and withdrawing: There are centres which were authorised to train people but suddenly they faced de-recognition, without giving an alternative to students for keeping their certificates. It has added in confusion and mal-practice both.
Issue raised in aftermath of statement given by honourable Minister Mrs Maneka Gandhi:
I have collected few of questions raised by activists in television shows and news-papers and trying to answer them appropriately.
- Sex policing not acceptable: To know the sex of baby is right of parents and is a medical requirement. It also helps in getting evidence of wrong doing! To ensure the health of a baby and protect her from unlaw-ful activity is the duty of government. Intermittent random check will obviate the need of one to one enquiry.
Tracking is not possible: I request all those who think that tracking cannot be done to go through upgraded sites of government of India, PCPNDT 2015. They have mentioned about cash reward for first informer and checking and tracking of all mothers upto the birth of child, by ASHA worker who keep, birth and MTP records. Even home delivery is conducted officially nowadays in many states.28It is done under the program "Safe Motherhood". In few states excelling in program like MP, a software "Mother and child tracking and recording" is in place and 98% deliveries are institutionalised under the "Janani Express Yojna".29
If a mother wants to abort baby for other reasons and it happens to be a girl child: Nowadays, pregnancy is detected early and upto 12 week there must be no consideration about sex. Because atleast USG can not accurately assign sex .
Biased family will ill treat the mother and unborn baby: If family is intended to do it, the situation after birth of baby with unidentified sex will remain same or will be culminated into female infantiside. The antenatal period must be used to give psychotherapy to the family with dubious record. However, it is most condemning argument to defend the PCPNDT chauvinist mentality.
Perfect-Handling of Issue-
Justify PCPNDT Act and its alternatives by Evidence based studies
Was it only Stringent anti-Ultrasound campaign or a positive atomosphere secondary to awareness campaingn and schemes for the girls, which made a little difference?
All controversial government programs must go through the scientific evaluation and new ideas must be felicitated. There is no published study to support positive and direct effect of PCPNDT on improving sex ratio. These kind of studies need public scrutiny because the improving sex ration in states like Rajasthan, once grossly infested with female infanticides from day back to 17th century, is not falling back to same practice after government control on female feticide, suggests change in 'mind set' secondary to improving awareness, media coverage and hope of better future for girls. There are so many students and medical colleges running research projects. Assigning few pilot projects to them will bring awareness and also scientific data to support hypothetical assumptions on either side.
Conclusion
It is satisfying that PCPNDT Act has worked on social aspects. Recent discussions in various forums has shown that once known as revolutionary, PCPNDT Act is now falling on traditional arguments, by ill-informed activists who are totally ignorant of enormity of damage done to critical care medicine by avoiding mobile ultrasound units. However, the recent government sites display the plans more than clerical record keeping which includes cash reward for informers, a decoy based surveillance, and maintaining the maternal and child tracking soft ware as well as keeping the MTP records by ASHA workers.27-30 Experts in Madhya Pradesh have claimed 98% institutionalized delivery after the onset of "Janani Express Yojna". Asking for a better record keeping from doctors is appropriate. However, equating it to dowry law is uncalled for!
Government and activists need to avoid extrapolation of few criminal acts by those who have criminal tendencies and harbour within the medical fraternity, to blacken entire medical profession.
Better respect of women, property rights, job preference for daughter from girl only family, pension schemes, state own cremations for parents in absence of any other family members, are the long term measures which will work positively for nation and particularly in north and central India.
Finally, PCPNDT Act was brought into, to tackle an emotional and social issue which reached up to the proportion of unmindful homicide with the help of medical fraternity, must not be a knee jerk emotional reaction but must be kept under well designed trials and studies before proclaiming its success.
(Acknowledgement : I am grateful to Dr Pratik Mittal ,DNB (Pediatrics) for editing of this document.)
REFERENCES
1.PCPNDT Act 1994 http://pndt.gov.in/writereaddata/mainlinkFile/File50.pdf
- Mishra Smita . PCPNDT Act vis a vis Point of care ultrasound (POCUS); January - April 2013 Journal of Indian Academy of Echocardiography
Chawla Vineeta: Where Are The Girls? Female Infanticide In Indiahttp://www.youthkiawaaz.com/2010/12/female-infanticide-in-india-2/
PCPNDT case: Bail for four Ruby Hall doctors: http://www.indianexpress.com/news/pcpndt-case-bail-for-four-ruby-hall- doctors/973319
SexTest: Arrest of 3 Kolhapur agents opens up can of worm- http://www.dnaindia.com/pune/report-sex-tests-arrest-of-3-kolhapur-agents- opens-a-can-of-worms-1709130
Dean AJ, Breyer MJ, Ku BS, Mills AM, Pines JM. Emergency ultrasound usage among recent emergency medicine residency graduates of a convenience sample of 14 residencies. J Emerg Med. 2010 Feb;38(2):214-20, quiz 220-1. Epub 2008 Aug 23.
Sarkisian AE, Khondkarian RA, Amirbekian NM, Bagdasarian NB, Khojayan RL, Oganesian YT. Sonographic screening of mass casualties for abdominal and renal injuries following the 1988 Armenian earthquake.J Trauma. 1991;31(2):247-250.
Rempell J. Point-of-care ultrasound training for Rwandan physicians and its impact on patient management Physicians Ultrasound in Rwanda Education Initiative (PURE)http://phsglobalhealth.blogspot.in/2012/03/physicians-ultrasound-in- rwanda.html
Sex selection: The forgotten story:BBC- http://www.bbc.com/news/14213136
AIIMS, New Delhi accused of promoting sex selection http://kriticulture.blogspot.in/2011/07/aiims-new-delhi-accused-of-promoting.html
Mishra Smita . PCPNDT Act vis a vis Point of care ultrasound (POCUS); January - April 2013 Journal of Indian Academy of Echocardiography
Woo J. A short History of the development of Ultrasound in Obstetrics and Gynecology http://www.ob-ultrasound.net/history1.html
Hsiao CH, Wang HC, Hsieh CF, Hsu JJ. Fetal gender screening by ultrasound at 11 to 13(+6) weeks.ActaObstetGynecol Scand. 2008;87(1):8-13.
Medical termination of pregnancy act 1971 :http://cfw.ap.nic.in/pdf/MTPAct1971.pdf
In the high court of judicature at bombaycivil appel late jurisdiction writ petition no.7896 of 2010 along with civil application no.512 of 2011http://bombayhighcourt.nic.in/data/judgements/2011/cwp2386710.pdf
Use of portable ultrasound machine banned. http://www.dnasyndication.com/dna/article/DNPUN47958
Union Government reconstituted Central Supervisory Board set up under PC & PNDT Act: http://www.jagranjosh.com/current-affairs/union-government-reconstituted- central-supervisory-board-set-up-under-pc-pndt-act-1302522527-1
Mallik R; 'negative choice'sex determination and sex selective abortion in india; http://www.cehat.org/go/uploads/AapIndia/work6.pdf
SaravananS : Violence Against Women in India A Literature Review ; March 2000; http://www.iss india.org/PDF/Violence%20Against%20Women%20India.pdf
Sekher TV and Hatti N; Vulnerable Daughters in a Modernizing Society: From 'son Preference' to 'daughter discrimination' in modern India; http://pndt.gov.in/writereaddata/mainlinkfile/File117.pdf
Maternal Blood Test Can Tell Parents Fetus's Sex After 7 Weeks, National Institutes of Health (NIH) Study; http://www.biospace.com/News/maternal-blood-test-can- tell-parents-fetuss-sex/229750/source=Featured
Devaney SA; Palomaki GE,; Scott JA, Bianchi DW, NoninvasiveFetal Sex Determination Using Cell-Free Fetal DNA :A Systematic Review and Meta-analysis; JAMA. 2011;306(6):627-636. doi:10.1001/jama.2011.1114
Ramzi's method of sexdetermination in 6th week of pregnancy: http://pregnancy.about.com/od/genderpredictions1/ss/Ramzis-Method-To- Determine-Fetal-Gender.htm
Malpani A, Malpani A, Modi D;Preimplantation sex selection for family balancing in India; Hum. Reprod. (2002) 17 (1): 11-12.
B.O Igbinedion, T.O. Akhigbe; The accuracy of 2D ultrasound prenatal sex determination; Niger Med J. 2012 Apr-Jun; 53(2): 71–75.
Mishra Smita. Anathema of Ultrasound; 2012; http://www.colordopplermedia.com/june/
Female Feticide: Enforce the Law, Get Safe Ultrasound Technology, Say Experts –Indian American Times http://indiaamericatoday.com/article/female-feticide- enforce-law-get-safe-ultrasound-technology-say- experts#sthash.oIRV9YyD.dpufhttp://indiaamericatoday.com/article/female- feticide-enforce-law-get-safe-ultrasound-technology-say-experts
PCPNDT ACT: http://www.pyaribitiya.in/
Janani Express Yojna MP:http://www.archive.india.gov.in/citizen/health/viewscheme.php?schemeid=2055
Rajasthan starts Informer Scheme to check sex selection dna.http://www.dnaindia.com/india/report-rajasthan-starts-informer-scheme-to-check- sex-determination-tests-2122467
Written by
Dr Smitha Misha
Associate Director, Jaypee Hospital, Noida
Chairperson, Cardiology Chapter of IAP
Disclaimer: This website is primarily for healthcare professionals. The content here does not replace medical advice and should not be used as medical, diagnostic, endorsement, treatment, or prescription advice. Medical science evolves rapidly, and we strive to keep our information current. If you find any discrepancies, please contact us at corrections@medicaldialogues.in. Read our Correction Policy here. Nothing here should be used as a substitute for medical advice, diagnosis, or treatment. We do not endorse any healthcare advice that contradicts a physician's guidance. Use of this site is subject to our Terms of Use, Privacy Policy, and Advertisement Policy. For more details, read our Full Disclaimer here.
NOTE: Join us in combating medical misinformation. If you encounter a questionable health, medical, or medical education claim, email us at factcheck@medicaldialogues.in for evaluation.